Augmenting clinical reasoning, without replacing it
On building AI tools that supercharge physicians' thinking while keeping them in control

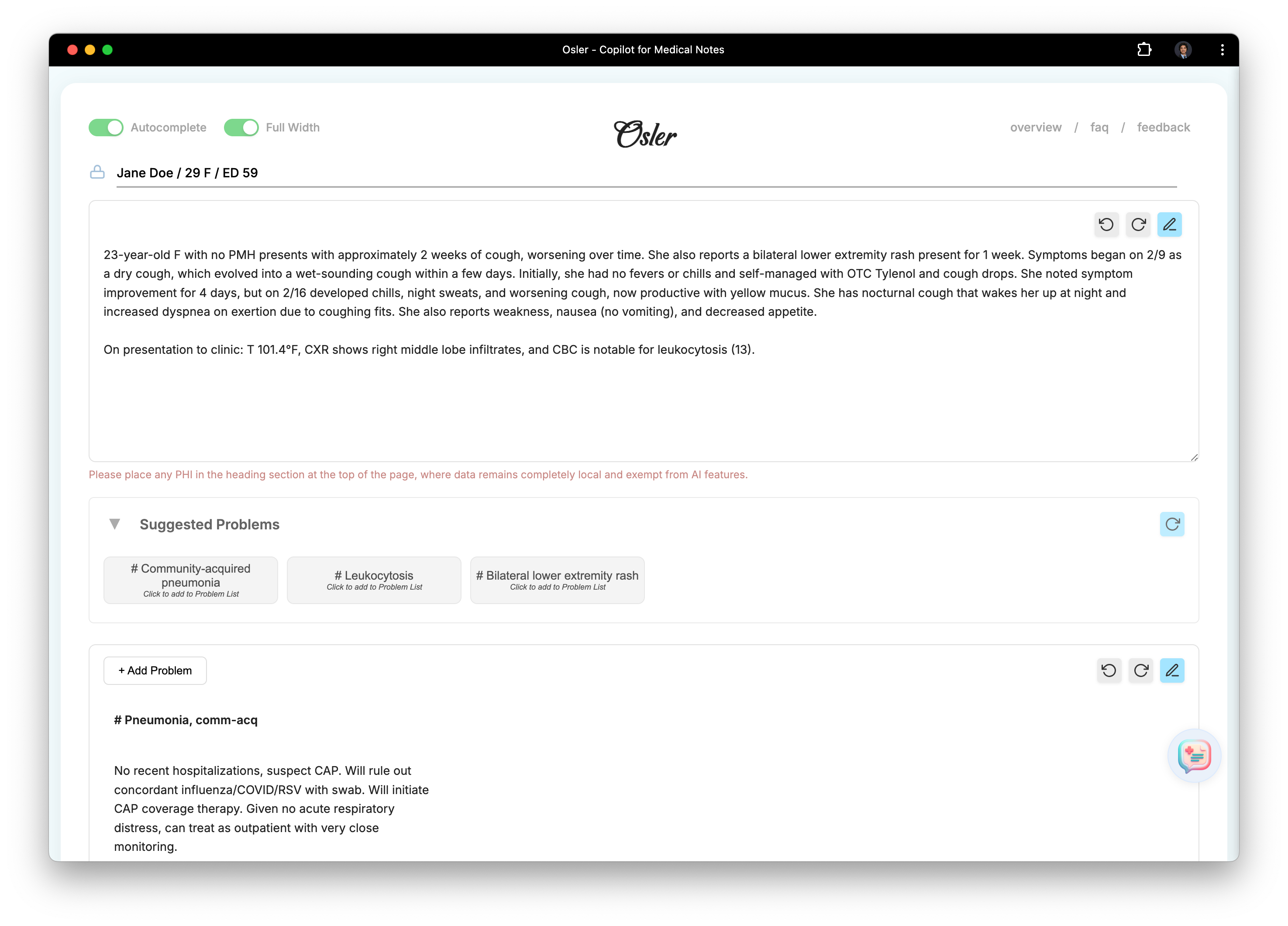
I recently launched Osler, a workspace and copilot designed for physicians writing History & Physical (H&P) notes.
As a resident physician, I built Osler around two guiding principles:
The act of writing notes helps doctors think and plan.
Great notes should enable clear, concise communication.
I’m a strong believer that the shape of tools impacts the thinking process, whether it’s writing code or performing clinical decision making (back in undergrad I spent years optimizing my Emacs config).
With a growing number of AI-based clinical tools (which have varying degrees of direct impact into the clinical workflow), I wanted to share my intuitions about how tools that augment physicians should look and behave. These thoughts have largely been refined through working as a resident physician and dogfooding the software I’ve built, observing areas where my workflow was optimized, and iteratively refining.
With that being said, I’d love to hear others’ experiences and thoughts, so please reach out to chat (X / email) if you have any you’d like to share!
I. Augmenting reasoning without replacing it
Over the past year, there have been a range of clinical AI tools that have gained adoption in clinical practice, with the goals of helping offload the note-writing burden for physicians.
One concern I have with many of these systems is that with LLMs, the boundary between specific task completion and reasoning is blurry. This is not always a bad thing — much of the value of these systems comes from doing reasoning — but the issue is when that reasoning starts to happen quietly in the background, without the clinician realizing where the conclusions came from. I’ve written about this in a little bit more detail, with some examples, here.
There are clear areas where AI can augment clinicians — I’ve benefitted from several of these! Some concrete examples:
offering differential diagnoses/workup that I may have not considered
determining whether my plans follow latest guidelines
identifying and clarifying ambiguity in my plans
I originally built Osler without any AI functionality, more as a notepad to structure my clinical writing (and by extension, my thinking), and therefore wanted to be very intentioned about how AI fit into the workflow. The current implementation is simultaneously deeply embedded within the current clinical context, but also ensures the final reasoning is in the hands of the clinician.
In practice, using Osler feels like the right balance of augmenting my clinical reasoning without losing control to AI.
I've been surprised by the sheer degree of value in being able to interrogate my thinking in real-time while writing a note, with responses contextualized to the specific clinical case, and suggestions I can easily accept/reject.
II. Building a net-useful clinical workflow outside of current EHR systems
There's always friction in building clinical tools that are distinct from the underlying monolithic EMR system — much of the daily clinical workflow has been crafted around existing tools (like the Epic EMR), and there can be a cost to adding something to that workflow.
Osler is designed to slot into existing clinical workflows as seamlessly as possible, while maintaining a distinct platform that facilitates more flexibility and ability to ship updates quickly. In my use at least, the considerable gains in speed, reasoning, and overall quality of notes I experience with Osler significantly outweigh value from EMR-specific features (like dotphrases or smartphrases).
The workflow with Osler is pretty straightforward: pull up Osler on any computer next to the EMR, use Osler as you think through the new admission, and then hit “Export” to easily paste the note into any EMR.
More broadly, I think this paradigm of AI tools that sits right outside existing workflows will continue to flourish, because the rapid progression of AI tools will outstrip how quickly end-to-end clinical workflows are able to adapt.
III. Moving forward
I’ve been excited to hear feedback from others on areas where Osler has brought real gains to their clinical workflow. If you’re interested to try the tool, it’s available for free at https://getosler.com/ — and I’d love to hear your thoughts!
